Complex Reconstruction of Chronic Pharyngocutaneous Fistula
Explore complex head and neck reconstruction case and advanced ENT surgical strategy.
3/1/20262 min read
Introduction
Severe complications following cervical spine surgery can profoundly affect swallowing, airway safety, and overall quality of life. Among the most challenging complications is the development of a pharyngocutaneous fistula, often accompanied by persistent dysphagia and chronic infection. This Blog outlines the surgical management of a complex chronic pharyngeal defect after multiple failed repair attempts in other ENT Centers.
Clinical Background
Three years following a severe road traffic accident, a patient underwent cervical spine fixation. Within ten days post-operatively, she developed a devastating complication: persistent dysphagia associated with a pharyngocutaneous fistula. Over the next three years, she underwent three unsuccessful surgical repair attempts at other different centers. The cervical fixation plates were eventually removed due to suspected infection. Despite these interventions, the fistula persisted, and she remained dependent on a gastrostomy tube for enteral feeding, significantly impairing her nutritional status and quality of life.
Chronic pharyngeal fistula after cervical spine surgery is rare but complex, particularly when multiple revision surgeries have been performed. Dense scarring, altered anatomy, and chronic inflammation make definitive repair technically demanding.
Comprehensive Assessment and Diagnostic Evaluation
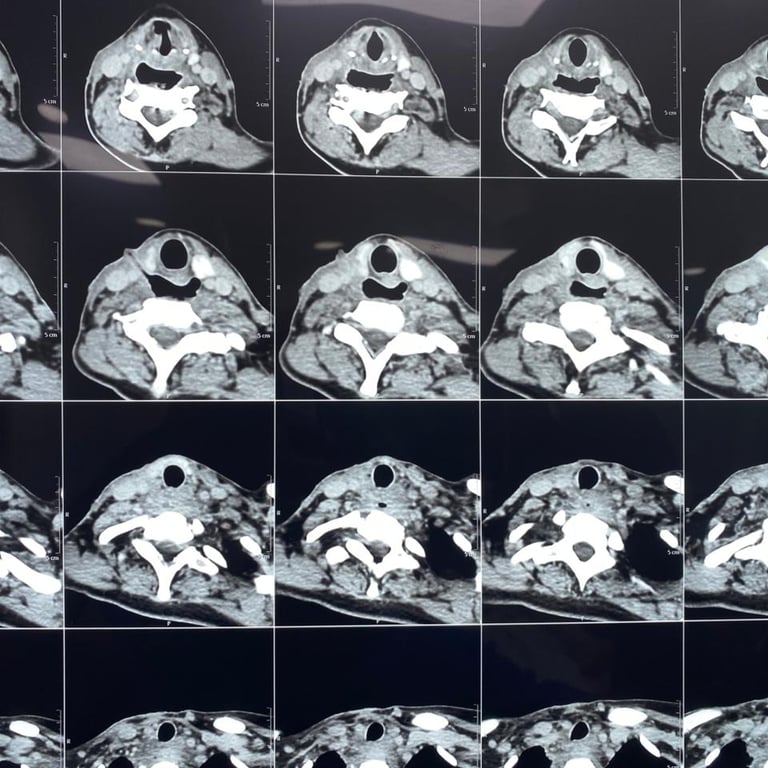
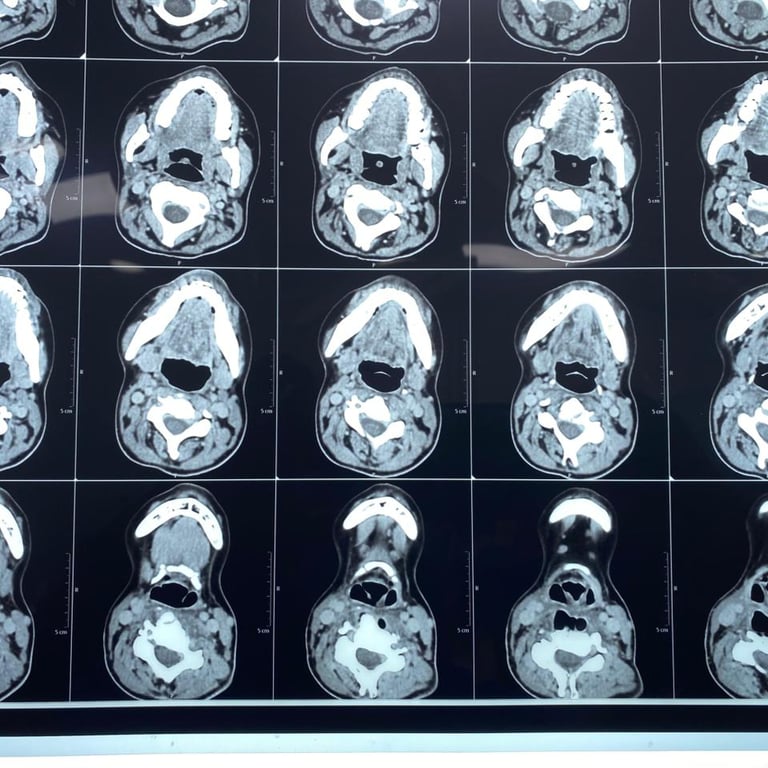
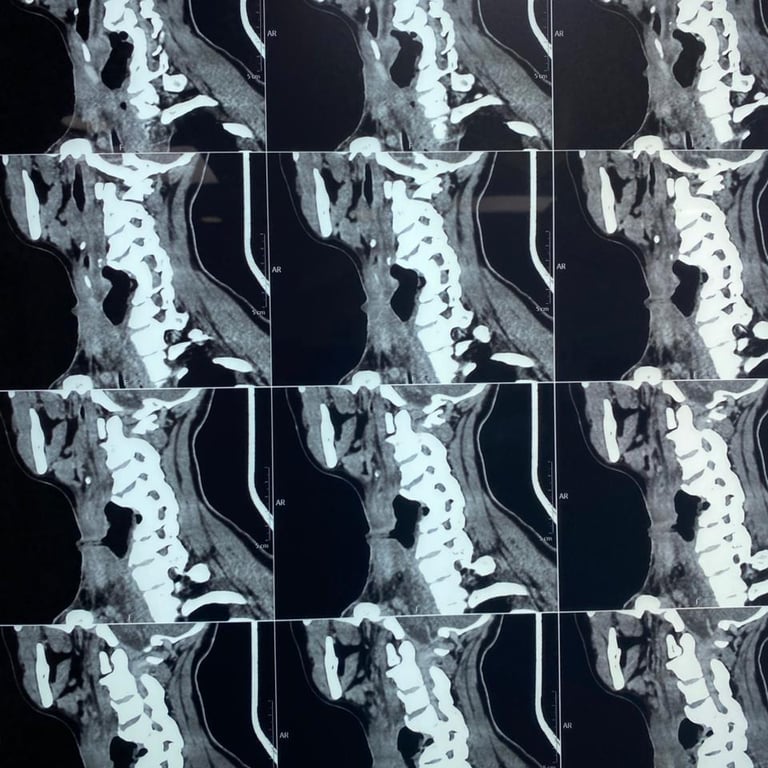
Upon presentation to me, a thorough clinical evaluation was performed, including endoscopic examination and imaging with CT and MRI.
In addition to confirming the chronic pharyngocutaneous fistula, imaging revealed a previously undetected large pharyngeal pouch, contributing to persistent leakage and impaired swallowing. Identifying this concealed pathology was critical to designing a definitive surgical strategy.
Multidisciplinary Surgical Strategy
Given the complexity of the case, a dedicated multidisciplinary surgical team was assembled. The surgical plan included:
Complete excision of the chronic pharyngocutaneous fistula
Exploration and definitive management of the pharyngeal pouch
Repair of associated pharyngeal defects
Reconstruction using a vascularized free flap for reinforcement and optimized healing
Pouch
Pouch exploration - Part 1

Pouch Opening
Pouch exploration - Part 2

Two Defects
Two defects exploration

Full Defect
Full defect exploration

After Repair
After repair exploration

Intraoperative Findings and Reconstruction
Intraoperatively, dense adhesions were encountered as a result of four previous operations (initial cervical fixation and three repair attempts). Repeated intraoperative endoscopic evaluations were necessary to accurately localize the pharyngeal pouch opening and define the full extent of the defect.
The pouch was successfully excised, and an additional pharyngeal defect was identified and repaired. To enhance healing and reduce recurrence risk, a well-vascularized free flap was utilized as a reinforcement layer, providing robust tissue coverage in a scarred surgical field.
Microvascular reconstruction plays a pivotal role in complex head and neck revision surgery, particularly in chronically infected or irradiated tissues.
Outcome and Functional Recovery
Postoperatively, the patient demonstrated progressive improvement in swallowing function.
The gastrostomy tube was successfully removed
Oral feeding was fully restored
Nutritional autonomy was regained
Quality of life significantly improved
Contact
Reach out anytime for appointments or questions
Phone
© 2026. All rights reserved. The website is developed by: Rosaline Makar
Subscribe to Our Newsletter